Common Sales Strategies
Because of these three things, I in turn see the same strategies used in business to drive profits again and again shape the practice of medicine.
For example, a profitable business is built around ensuring recurring sales of high margin products. One way to describe the vaccine program is that the CDC’s schedule is a vehicle for ensuring that, as once a vaccine is on the CDC’s schedule, millions of annual sales are guaranteed in the US alone.
Note: typically the most aggressive promotion is for the vaccines with the highest profit margins (e.g., the annual adult vaccines or the HPV vaccine).
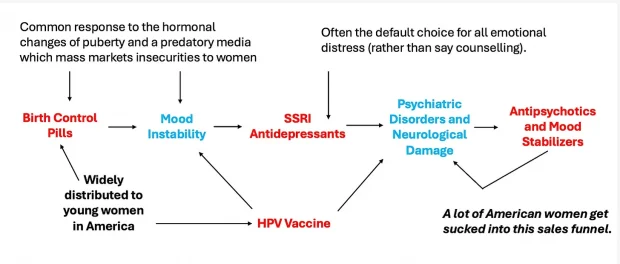
Similarly, much of business revolves around creating sales funnels where a low entry (and often free) product is offered, to gradually pull customers into buying progressively more expensive ones. In healthcare, I’ve gradually gained appreciation for how much of the practice of medicine are simply regimented sales funnels (e.g., one of the primary purposes of “wellness” bloodwork screenings are to sell harmful drugs like statins to patients), and likewise, many drugs have a myriad of side effects which then require progressively more expensive drugs to treat. For example, as I discussed in a recent article about the danger of antidepressants, this is a common sales funnel I see affect many girls in America:
Note: a strong case (discussed further here) can also be made that the childhood vaccine program is responsible for many of the chronic illnesses in America—which coincidently is also one of the largest markets for the pharmaceutical industry. Likewise, we are now seeing that companies like Pfizer are focusing on developing new drugs which treat the side effects of COVID-19 vaccines.
Another common strategy is to protect large potential markets by keeping any product that could threaten it off the market. Most recently, we witnessed the government (and many others) do this by demonizing affordable and effective COVID-19 treatments so that a myriad of ineffective, costly and often harmful products (e.g., remdesivir and the vaccines) could monopolize the COVID-19 market. However, this sadly is by no means an isolated incident. For example, I’ve previously discussed how:
•In the 1940s, Ultraviolet Blood Irradiation, a miraculous therapy was rapidly adopted by hospitals throughout America because it made a variety of otherwise fatal and incurable illnesses curable. After its inventor refused to give away the rights for it to the American Medical Association, the AMA buried it so that a competing therapy, antibiotics, could take over the market place.
•During the AIDS crisis, Fauci (and the FDA) did everything they could (including defying Congress) to prevent effective treatments for AIDS from hitting the market so that he could instead get a lucrative (but dangerous and ineffective) pharmaceutical approved and enshrined as the definitive “treatment” for AIDS.
•In the early 1990s, a remarkably safe and effective treatment for insomnia (GHB) began being used throughout America and frequently produced life changing results for patients with a variety of chronic illnesses (as healthy sleep is essential for health)—which unfortunately meant it was an existential threat to the multibillion sleeping pill industry. Since the evidence for GHB was very strong and it was a natural supplement (meaning the FDA had no statutory authority over it), the FDA instead decided to remove by conducting a series of illegal raids against suppliers of it, and then once the courts stopped that, the FDA pivoted to creating a non-sensical (and false) hysteria which resulted in Congress passing a law outlawing GHB which subjected the harshest penalties we have against anyone in possession of it.
•Almost all the research on the Alzheimer’s (which amounts to billions of dollars each year) is aimed at finding ways to eliminate the abnormal brain proteins found in Alzheimer’s disease, despite none of that research ever yielding anything which benefits patients, the pivotal paper in that field which justified all that research being proven to have been fraudulent and many researchers unsuccessfully petitioning for other lines of research. Likewise, there has been only one (un-patentable) therapy which was ever proven to reverse (cure) Alzheimer’s—yet almost no one knows it exists, despite Alzheimer’s costing the US over 300 billion dollars annually (making it the most expensive disease in America). Hence, that market has been “preserved,” best shown by the FDA recently pushing through two expensive drugs which were so ineffective and unsafe the FDA had to overrule its own panel to approve one (and backdoor the approval process of the other), which was immediately followed by the head of the FDA being the keynote speaker at the annual pharmaceutical investor’s conference (which focused on the immense future profitability of the Alzheimer’s drugs).
Likewise, consider these recent events:
For the past two decades, scientists, researchers, and veteran advocates have sought the answer to a burning question: Can MDMA-assisted therapy (MDMA-AT) provide a significantly better treatment option for PTSD than currently available treatments?
The urgency of this question is fueled by the fact that billions of dollars and over 20 years of research have done absolutely nothing to curb, much less end, our veteran suicide epidemic. Over 6,000 veterans, most of whom suffered from PTSD, have taken their own lives each and every year since 9/11. The cumulative loss to suicide is more than 130,000 veteran lives and climbing, a number 18 times greater than the 7,054 U.S. servicemembers’ who lost their lives in post-9/11 combat zones.
Note: PTSD also leads to many veterans being homeless.
The answer to the question of MDMA-AT’s efficacy thus provides a much-needed surge of hope: Phase Three clinical trial results have demonstrated that this treatment is both safe and efficacious. Seventy-one percent of trial participants, who suffered an average of 14 years from debilitating PTSD, no longer qualified for a PTSD diagnosis, while 86.5% experienced clinically significant improvement in their symptoms. These results are “almost double” the efficacy of existing treatments. If these results hold up outside clinical studies, it would render MDMA-AT the most effective PTSD treatment ever developed.
Over the past year and a half, MDMA-AT’s efficacy has garnered a slew of positive press, FDA “Breakthrough Therapy” designation and fast-tracked approval consideration, bipartisan support from policymakers, and government funding through both the Department of Defense and the Department of Veterans Affairs. MDMA-AT’s FDA approval, slated for August 11, 2024, thus seemed to be on the verge of materializing to the relief of millions of suffering veterans.
But earlier this spring, something changed in the media narrative. Articles with suspicious origins and strikingly similar narratives raised unfounded and almost laughable rumors, alleging that the 20-plus years of scientific research by the NIH, VA, prominent universities, and researchers were the work of a “cult.”
Surprisingly, these rumors emerged publicly at the June 4, 2024, meeting of an external FDA Advisory Committee, empaneled by the FDA to consider MDMA-AT’s merits. Rather than assess the data at hand, the Committee devolved into what one expert called a “dumpster fire.” The group strayed from analyzing the safety and efficacy of the treatment to asking bizarre questions about the diversity of the trials, the types of therapy used, and questions regarding whether MDMA-AT would lead to cocaine usage. No mention was made of the veteran suicide epidemic or the soundness of the clinical trials’ results. Consequently, the committee voted against recommending FDA approval of this FDA-designated “breakthrough therapy” that would provide life-saving relief to the 13 million Americans who suffer from PTSD today.
Leading scientists, policymakers, and veteran advocates watched the advisory committee meeting with confusion and disbelief. According to the BBC, Dr. Franklin King, a psychiatrist at Mass General Hospital and Harvard Medical School, observed that “advisory committee members really showed a kind of astounding lack of knowledge about the subject matter.” Dr. Natalie Gukasyan, an assistant professor of psychiatry at Columbia University Irving Medical Center, stated: “It’s almost like this came as a total surprise that this was the study design, when in fact the FDA approved this design.” Republican Congressman and retired Lieutenant General Rep. Jack Bergman (R-MI) said, “I’m disappointed that the FDA advisory committee chose to ignore the voices and testimonies of Veterans whose lives have been forever improved by MDMA-assisted therapy, and instead voted in favor of those who have been on a mission to discredit this promising treatment at all costs.” And former Navy SEAL, Republican Congressman Morgan Luttrell (R-TX), slammed the Committee’s vote as “stemming from a lack of education and experience around the clinical use of psychedelics.”
The question that needs to be asked is: who influenced the Advisory Committee, and why?
Weeks before the meeting, a group called ICER, which claims to “conduct evidence-based reviews of health care interventions,” published a draft report of a study that is critical of MDMA-Assisted Therapy and its sponsoring company, Lykos. ICER’s funders include insurance and pharmaceutical companies with a vested interest in preserving the status quo of healthcare. Its opposition to MDMA-AT is thus likely influenced by Big Pharma, which makes billions of dollars on antidepressants ($16.6Bn in 2023), which are largely ineffective treatments for PTSD.
Furthermore, one of the “experts” ICER relied on in drafting its report is an individual closely associated with a little-known group called Psymposia. This Individual has made it their stated mission to prevent MDMA-AT’s FDA approval due to their personal antipathy towards the therapy’s sponsor, Lykos. After the Advisory Committee’s vote, they publicly claimed victory as the engineer of ICER’s public crusade against MDMA-AT.
The motivation of many of the people associated with Psymposia for opposing MDMA-AT lies in their belief that treating veterans suffering from PTSD “perpetuates the logic of white supremacism, capitalism, and imperialism.” They openly refer to veterans as imperialists, white supremacists, and murderers on their website, in public speeches, and on their social media feeds. This hateful, anti-veteran rhetoric infiltrated the media and the Advisory Committee’s psyches through ICER’s draft report, as evidenced by how often committee members raised the issue of a perceived “lack of diversity” in MDMA-AT’s Phase 3 clinical trials. Moreover, they clung to this narrative despite the fact that over half of confirmatory Phase 3 trial participants self-identified as a race or ethnicity other than white or non-Hispanic Latino.
As veterans, PTSD advocates, and Americans, it is our responsibility to expose the underlying motives for the carefully coordinated, unscientific, anti-MDMA smear campaign. The Individual and their colleagues at ICER and Psymposia have successfully manipulated the media and infiltrated the FDA’s regulatory process to the detriment of millions. Psymposia’s involvement in ICER’s report should have rendered its “findings” null and void. Instead, it may single-handedly dash the hopes of thousands of veterans who continue to take their own lives due to their suffering from PTSD.
For this reason, and because of the overwhelming scientific evidence in favor of MDMA-AT’s efficacy, we urge the FDA and members of the media to take the Advisory Committee’s vote with a grain of salt. Too many lives are at stake for anything other than science to guide the FDA’s decision. Veterans’ lives are now dependent on the FDA’s ability to separate fact from opinion – especially ones that attack, rather than support, those who’ve risked their lives to protect and defend ours.
Note: a longstanding problem is how poorly America treats its veterans (e.g., I have friends who served in Vietnam who were left with severe PTSD or a myriad of Agent Orange induced cancers that unsuccessfully fought for decades to get help from the government and much of what they experienced is identical to what I now hear from Iraq and Afghanistan vets). Since the government frequently won’t help them with the basic things they need to function or heal, they often have to turn to the black market to get it instead (e.g., there are veteran networks for MDMA psychotherapy or GHB as both really help them). Conversely, colleagues for years have been working to advance the research showing MDMA (ecstasy) helps veterans with PTSD (as they recognize how great the need is here), but as the above example shows, all of that work is essentially irrelevant once a pharmaceutical company decides its turf has been threatened.
As best as I can tell, the reason the FDA always does this relates to another principle of business—to get investors, you need to be able to demonstrate that it is likely your investment with produce a return. Because of this, marginal products which have an established sales pipeline are the most frequent to enter the market, whereas unorthodox ones rarely gain support, regardless of their potential merit. For example, in Hollywood, because they are so many ways to make money from a movie (e.g., film merchandise or cable re-runs) a movie that fits into an existing franchise will easily attract investors (e.g., they are currently making Fast & Furious XI), whereas creative and non-standard scripts with the potential to be real blockbusters instead struggle to attract investors and get off the ground.
The post Pumping and Dumping Vaccines appeared first on LewRockwell.
0 comments on “Pumping and Dumping Vaccines” Add yours →